A major healthcare provider in the United States is facing intensifying scrutiny from its own clinicians, unions, and regulators over controversial changes to how it assesses patients seeking mental health care. The dispute centres on whether the drive for efficiency is compromising patient safety.
Clinicians Strike Over “Fundamental” Changes to Care
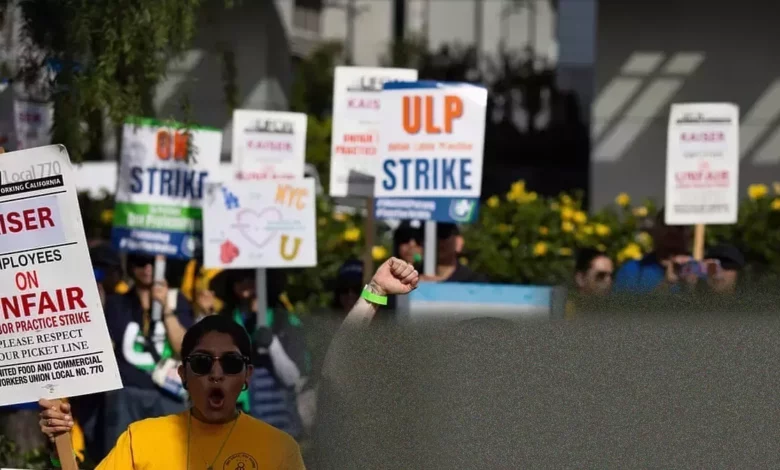
This week, approximately 2,400 mental health professionals employed by Kaiser Permanente in Northern California staged a 24-hour strike. Their action protests a new patient screening system and growing fears that artificial intelligence (AI) could replace licensed therapists for core clinical work. “Human work needs to stay with human beings,” said Ilana Marcucci-Morris, a licensed clinical social worker at Kaiser’s Oakland psychiatry clinic.
The strikers, represented by the National Union of Healthcare Workers (NUHW), allege that since January 2024, Kaiser has fundamentally altered the first point of contact for new patients. Where licensed professionals once conducted initial assessments, the union says clerical workers now ask scripted “yes” or “no” questions, while other patients are directed to online questionnaires, known as e-visits.
Kaiser Permanente firmly denies the union’s characterisation. In a statement, the healthcare giant said “AI and Clerical staff are not conducting any assessments, making any clinical determinations nor conducting clinical triage.” It added that clerical staff are trained to escalate cases immediately to a crisis therapist and that it is “growing our workforce, not shrinking it”. The company states its goal for AI is to support clinicians by reducing administrative work, not to replace human judgment.
Allegations of a Dangerous Bottleneck
Frontline therapists, however, report a system in distress. Five licensed Kaiser therapists told the Guardian that since the new process began, they have seen high-risk patients wait longer for care, while lower-risk cases are sometimes fast-tracked, clogging the system.
Carolyn Staehle, a therapist who started in Kaiser’s intake department in Pleasanton in May 2023, said that after the changes, she met many more people experiencing dangerous delusions or serious suicidal thoughts who should have been sent to emergency services much sooner. “They needed me to call an ambulance for them,” she said.
Now on a crisis team for higher-severity cases, Staehle says her unit is often dealing with “people who don’t need [us],” which slows down care for those in desperate need. Her concern is echoed by Marcucci-Morris in Oakland, who says she now often assesses severe cases and thinks: “Thank God they’re still alive.”
The NUHW has filed formal complaints with the California Department of Managed Health Care (DMHC) in both Northern and Southern California, alleging the new system is illegal. A complaint filed in April 2025 specifically accuses Kaiser of illegally using unlicensed clerical staff and a computer algorithm to triage mental health patients.
The union says clerical staff input patient answers into a software tool, the algorithm of which generates a score and suggests a response to guide scheduling. Kaiser denies this screening constitutes triage. According to an NUHW complaint, therapists have reported more than 70 examples of the system resulting in negative care outcomes since January 2025.
AI Anxiety and a Shrinking Specialist Workforce
Underpinning the dispute over screening is a deeper anxiety about automation. A 2025 internal survey of Kaiser’s Northern California mental health workers, obtained by the Guardian, found more than one-third feared the company had already rolled out AI or other technologies that could negatively affect work or patient care. Almost half expressed discomfort with introducing AI tools into clinical practice.
Specific concerns have been raised about AI software like Abridge, used for note-taking, regarding transparency and data retention. Kaiser states staff are not required to use Abridge, patient consent is obtained, and clinicians review all AI-generated notes. It is noted that Kaiser Permanente Ventures has invested in the Abridge company.
Concurrent with these technological shifts, clinicians report a reduction in specialist triage staff. Harimandir Khalsa, who does triage in Kaiser’s Walnut Creek facility, said her team of nine has been reduced by two-thirds over two years. The NUHW contends the number of triage therapists has decreased significantly, a claim Kaiser disputes.
Staffing retention is a broader issue. In Southern California, a substantial percentage of mental health professionals hired between 2021 and 2024 left their positions, many within their first year. Kristi Reimer, a licensed psychologist, said she pre-emptively left her triage role at the Walnut Creek facility because she saw “the writing on the wall” regarding the assessment system’s drastic change.
A History of Regulatory Penalties and Settlements
Kaiser’s mental health services have been under persistent regulatory scrutiny. In October 2023, the company agreed to a $200 million settlement with the California DMHC, including a $50 million fine, over delays in behavioural health services. This required Kaiser to invest an additional $150 million over five years in mental health initiatives.
More recently, in February 2026, Kaiser agreed to a $31 million settlement with the U.S. Department of Labor (DOL) over allegations it failed to provide timely access to mental health and substance use disorder services. The DOL claimed Kaiser “used patient responses to questionnaires to improperly prevent patients from receiving care.” A separate $28 million DOL settlement concerned reimbursing members for out-of-network care.
Other penalties include an $819,500 fine from the DMHC in April 2025 for late complaint processing, and a $46 million settlement in January 2026 over allegations of improper sharing of patient data through websites and apps.
The Human Cost of Automated Triage
Clinicians argue that nuanced, expert judgment is being lost. Triage is rarely straightforward, says therapist Harimandir Khalsa. Assessing suicide risk, for example, requires probing whether thoughts are active or passive, or if a method has been considered—complexities a scripted questionnaire or unlicensed worker may not capture.
The legal basis of the union’s complaint rests on California’s Health and Safety Code, which states mental health screening must be conducted by a physician, registered nurse, or other qualified health professional. The NUHW asserts Kaiser’s current model violates this.
For now, clinicians like Carolyn Staehle are focused on contract negotiations, seeking a guarantee that licensed professionals will not be replaced by AI. As she and her colleagues grapple with a transformed system, the fundamental question remains whether automated efficiency can ever replicate the critical, often life-saving, judgment of a trained therapist at a patient’s most vulnerable moment.