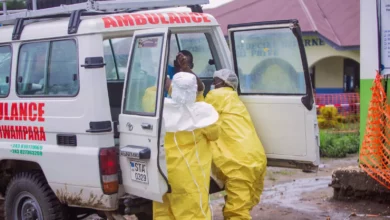
A proposed billion-dollar health financing deal between the United States and Zambia has sparked allegations of exploitation and raised serious concerns over data sovereignty and hidden economic agendas, according to a leaked draft agreement.
The draft five-year Memorandum of Understanding (MOU), worth over $1bn (£740m), would see Washington provide $1.012bn in health funding. In exchange, Zambia would be required to hire 40,000 new health workers, contribute an additional $400m of its own funds to health services, and meet strict performance targets. Failure on any front could see the US terminate the agreement and withdraw its funding.
Terms “Vastly Worse” Than Other Deals
Critics argue the terms are significantly more demanding than those the US has reached with 16 other African nations. A major point of contention is a commitment to give Washington access to Zambian health data for 10 years—far longer than other countries have negotiated. Furthermore, Zambia would be required to provide information on any new or emerging pathogens within its borders for the next 25 years, a clause not found in other publicly available MOUs.
“This is essentially our Zambian government signing away the right to access health data of its citizens to another country,” said Josiah Kalala, director of the Chapter One Foundation, a Zambian human rights organisation.
The controversy extends beyond data. In early December, the US embassy in Zambia confirmed the health financing was contingent on “collaboration in the mining sector and clear business-sector reforms” to improve US economic access. The MOU commits the Zambian government to monthly briefings with the US embassy aimed at “expanding US commercial investment in Zambia.” The US Assistant Secretary of State for Economic, Energy, and Business Affairs, Caleb Orr, has reportedly met with Zambia’s mines ministry and US mining firms operating in the country.
Asia Russell, director of the HIV advocacy organisation Health Gap, accused the US of “shameless exploitation.” She stated, “These terms are vastly worse than other deals. [The US] is conditioning life-saving health services on plundering the mineral wealth of the country.”
A Shifting US Strategy and Regional Ripples
The Zambia deal is part of a broader shift in US global health strategy under the Trump administration, often termed an “America First” approach. This strategy channels financing directly to governments instead of through aid organisations, while demanding increased co-investment from partner countries. It has coincided with the dismantling of much of the federal development agency, USAID.
This new model is already causing friction elsewhere. Last Wednesday, Zimbabwe said it was halting its own bilateral health agreement talks with the US, deeming the offer an “unequal exchange” and citing concerns over sharing sensitive health data.
For Zambia, the proposed US commitment of $1.012bn over five years is lower than the $1.5bn agreement that the country’s then-health minister, Elijah Muchima, announced in November 2025. It also represents a reduction: the US committed $367m to Zambia for HIV services alone the previous year, whereas the total annual health funding for 2026 under the draft MOU would be $320m, covering HIV, malaria, TB, and disease surveillance.
Political Fallout and Domestic Pressure in Zambia
The deal has caused political turbulence within Zambia. On 15 February, Health Minister Elijah Muchima denied on television that health financing was linked to mining concessions, stating, “If there are other external conditions attached, I am personally not part of that.” He was fired by President Hakainde Hichilema three days later without explanation.
Civil society groups, alarmed by the potential risks, are mobilising. Julius Kachidza, chair of Zambia’s Civil Society Self-coordinating Mechanism and a person living with HIV, supports goals like improved services but fears the consequences of failure. “If the HIV programme in Zambia is distorted or it’s disrupted or it’s derailed, I’ll be the first casualty,” he said, describing the situation as like “being held hostage.”
Activists secured a meeting with the health ministry on 3 February, but officials reportedly warned against legal action over data-sharing and refused to clarify if funding was tied to economic concessions. The groups are now demanding the removal of data-sharing requirements and a seat on the deal’s steering committee. Kalala is also pursuing an access-to-information request to make the latest versions of the MOU public, stating, “Once we get sight of the agreement and the compact, we’ll even be able to see if we can challenge the constitutionality of some of the provisions.”
The Zambian government faces a difficult calculus. The country’s 2026 budget for health services is roughly $1.3bn, but over a third of the national budget is consumed by debt repayments. Kalala suspects the government is proceeding partly due to a “major concern about the sudden loss of funding to the health sector and the political fallout that might cause.”
A US State Department spokesperson declined to discuss the MOU’s details but said in a statement, “The administration believes that American foreign assistance must demonstrably advance American national interests and use taxpayers’ dollars efficiently.” The Bureau of Global Health Security and Diplomacy, which has been negotiating the agreements, did not respond to requests for clarification. Zambia’s Ministry of Health did not respond to requests for comment.
The MOU includes a clause that the entire process will be terminated if an agreement is not reached by 1 April, setting a hard deadline for the resolution of a deal that has become a flashpoint for concerns over sovereignty, data rights, and the future of international health aid.